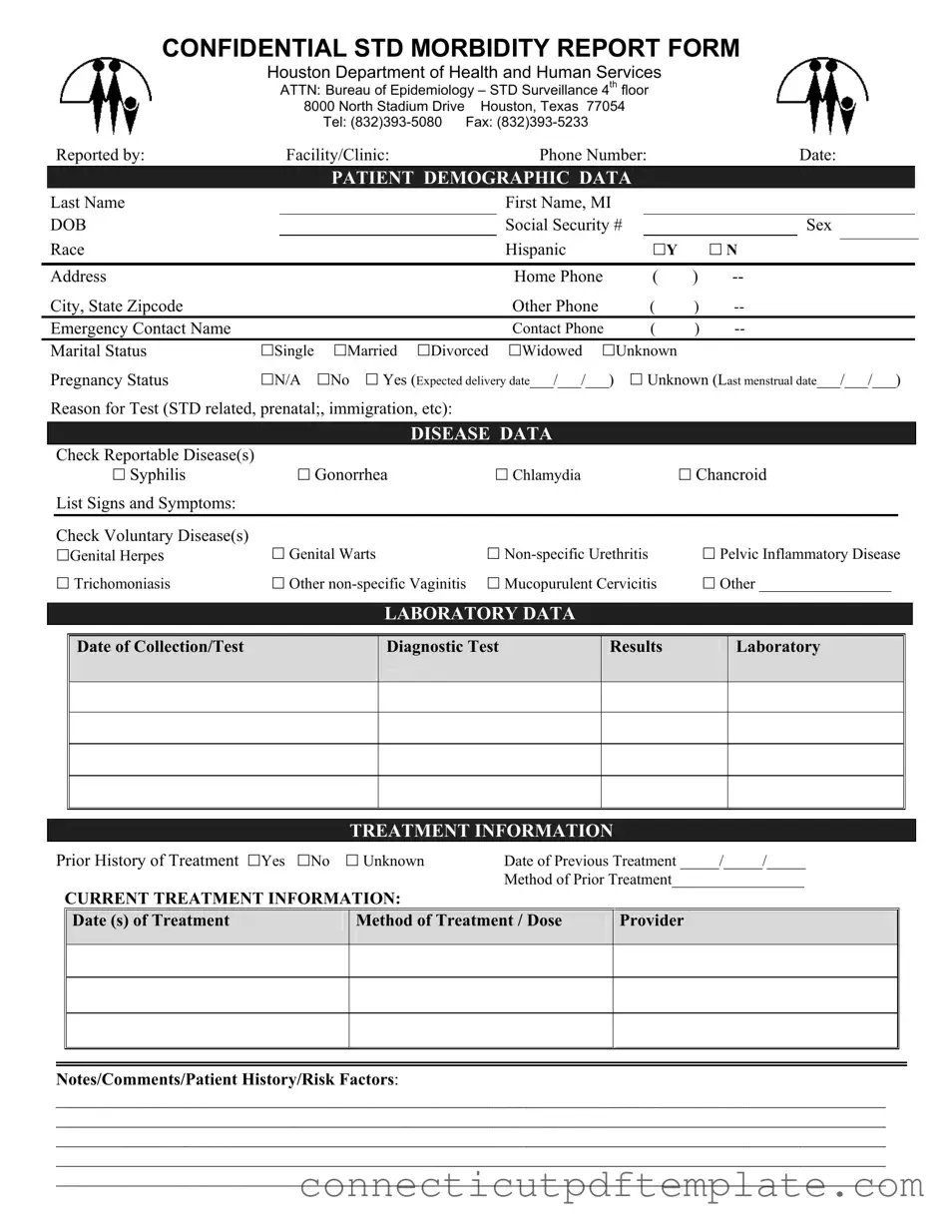
The Connecticut UC 2 form plays a vital role in the reporting and tracking of sexually transmitted diseases (STDs) within the state. This confidential morbidity report is specifically designed for healthcare providers to submit essential patient information to the Bureau of Epidemiology at the Houston Department of Health and Human Services. The form captures a wide range of data, starting with patient demographics, including names, contact information, and social security numbers. It also addresses critical aspects such as the patient's marital status and pregnancy status, which can be significant in understanding their health context. Furthermore, the form requires the reporting of specific diseases, allowing healthcare professionals to check off reportable STDs like syphilis, gonorrhea, and chlamydia, as well as voluntary diseases like genital herpes and pelvic inflammatory disease. Laboratory data, including the date of collection and test results, is also documented to ensure accurate tracking of disease trends. Treatment information is a key component, detailing any prior treatments and current methods, which helps in assessing the effectiveness of care provided. Overall, the Connecticut UC 2 form serves as a crucial tool for public health surveillance, enabling better management and prevention of STDs across the state.
CONFIDENTIAL STD MORBIDITY REPORT FORM
Houston Department of Health and Human Services
ATTN: Bureau of Epidemiology – STD Surveillance 4th floor
8000 North Stadium Drive Houston, Texas 77054
Tel:
|
|
Reported by: |
|
Facility/Clinic: |
|
Phone Number: |
|
|
Date: |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
PATIENT DEMOGRAPHIC DATA |
|
|
|
|
|
|
|||||
|
Last Name |
|
|
|
|
|
First Name, MI |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DOB |
|
|
|
|
|
Social Security # |
|
|
|
Sex |
|
||||
|
Race |
|
|
|
|
|
Hispanic |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
Y |
|
N |
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
Home Phone |
( |
) |
|
|
|
|
|||
|
City, State Zipcode |
|
|
|
|
|
Other Phone |
( |
) |
|
|
|
|
|||
|
Emergency Contact Name |
|
|
|
|
|
Contact Phone |
( |
) |
|
|
|
|
|||
|
Marital Status |
Single |
Married |
Divorced |
Widowed |
Unknown |
|
|
|
|
|
|
||||
|
Pregnancy Status |
N/A |
No |
Yes (Expected delivery date___/___/___) |
|
Unknown (Last menstrual date___/___/___) |
|
|||||||||
|
Reason for Test (STD related, prenatal;, immigration, etc): |
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DISEASE DATA |
|
|
|
|
|
|
|
|
|
|
|
Check Reportable Disease(s) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Syphilis |
|
|
Gonorrhea |
|
Chlamydia |
|
|
Chancroid |
|
|||||
|
|
List Signs and Symptoms: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Check Voluntary Disease(s) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Genital Herpes |
|
Genital Warts |
|
|
|
Pelvic Inflammatory Disease |
|
|||||||
|
|
Trichomoniasis |
|
Other |
Mucopurulent Cervicitis |
|
Other _________________ |
|
||||||||
LABORATORY DATA
Date of Collection/Test
Diagnostic Test
Results
Laboratory
TREATMENT INFORMATION
Prior History of Treatment Yes No |
Unknown |
Date of Previous Treatment _____/_____/_____ |
|
||
|
|
|
Method of Prior Treatment_________________ |
|
|
|
CURRENT TREATMENT INFORMATION: |
|
|
|
|
|
Date (s) of Treatment |
Method of Treatment / Dose |
Provider |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Notes/Comments/Patient History/Risk Factors:
_________________________________________________________________________________________________
_________________________________________________________________________________________________
_________________________________________________________________________________________________
_________________________________________________________________________________________________
_________________________________________________________________________________________________
| Fact Name | Description |
|---|---|
| Purpose | The Connecticut UC 2 form is used to report confidential morbidity related to sexually transmitted diseases (STDs). |
| Governing Law | This form is governed by the Connecticut General Statutes, specifically Section 19a-215. |
| Confidentiality | Information provided on this form is confidential and protected under state privacy laws. |
| Who Reports | Healthcare facilities and clinics are responsible for submitting this form when reporting STD cases. |
| Demographic Data | The form requires detailed patient demographic data, including name, date of birth, and address. |
| Laboratory Data | Laboratory results, including the date of collection and diagnostic test results, must be documented. |
| Treatment History | Prior treatment history is crucial, including dates and methods of any previous treatment. |
| Current Treatment | Current treatment information must be provided, including dates and methods of treatment. |
| Emergency Contact | The form requires an emergency contact's name and phone number for the patient. |
| Reporting Deadline | Reports should be submitted promptly, as required by state law, to ensure timely public health responses. |
How to Transfer Ownership of a Car to a Family Member in Ct - Includes space for the authorized municipal official's signature, providing legal authorization for the actions taken.
Ct Dmv Registration Requirements - A critical benefit for Connecticut-based military personnel, aiming to alleviate some financial pressures.
For those seeking clarity in their rental agreements, understanding the California Lease Agreement form is crucial. This document ensures that both tenants and landlords are aware of their rights and obligations, facilitating a smoother renting process. To learn more about the specifics, consider visiting a reliable source for Lease Agreement guidance.
Injured Spouse Form - Filers must remember to check the box for Form CT-8379 on their Connecticut return.